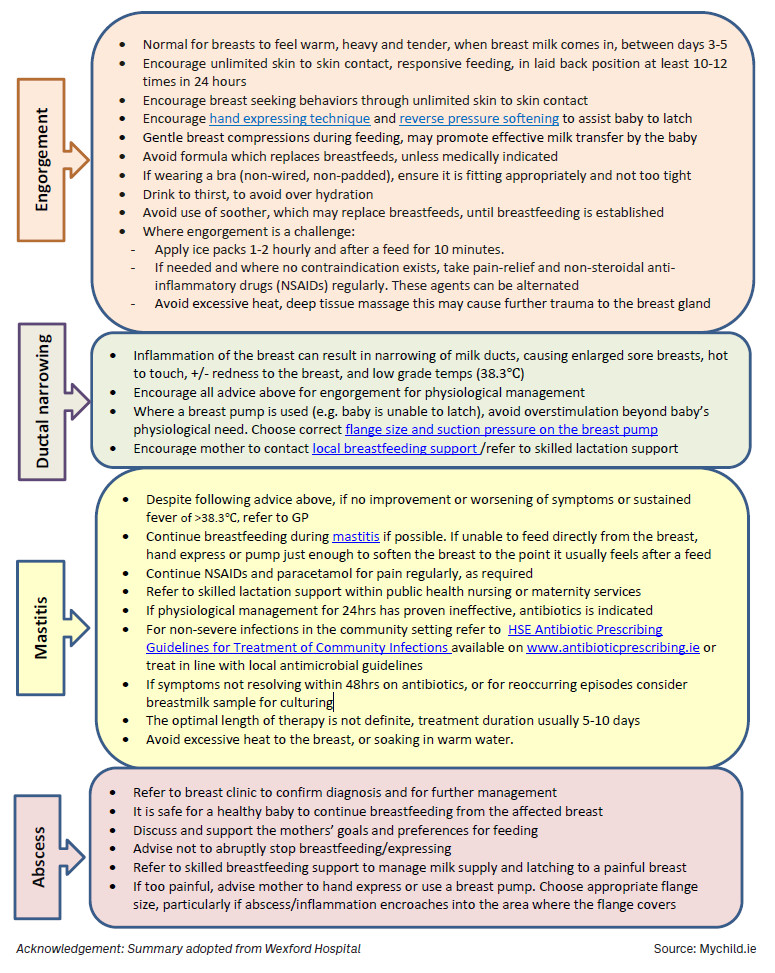
Mastitis is a common complication experienced by breastfeeding mothers which can result in the early cessation of breastfeeding. As healthcare professionals who are often the first point of contact for mothers seeking advice, pharmacists are uniquely positioned to play a meaningful role in the early recognition and appropriate management of this condition. An understanding of current evidence-based guidelines is essential for delivering informed and effective care:
Figure 1: Mastitis symptoms
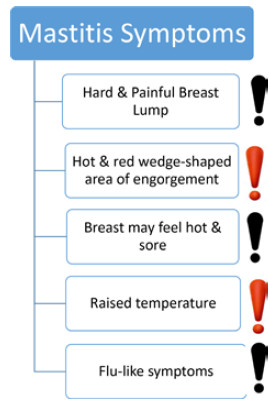
Mastitis is often caused by hyperlactation or temporary engorgement of a region of breast tissue. It is usually inflammatory rather than a bacterial infection. Therefore, non-pharmacological measures are often the most appropriate interventions initially.
Figure 2: Non-pharmacological treatment measures
Pharmacists are well placed to educate the mother on the importance of these non-pharmacological interventions measures.
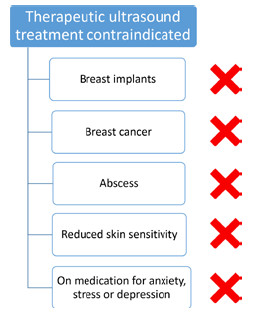
Therapeutic ultrasound treatment uses high-frequency sound waves and thermal energy to penetrate deep into the tissues, reducing inflammation and swelling. Therapeutic ultrasound treatment can be performed every three to four days to help symptoms resolve. See Figure 3 for contraindications of therapeutic ultrasound treatment.
Figure 3: Contraindications of therapeutic ultrasound treatment
Both the ABM protocol and HSE guidelines are unequivocal in their recommendation that breastfeeding should continue during an episode of mastitis. Cessation of feeding increases the risk of milk stasis, abscess development and prolonged illness. Mothers should be reassured that continued breastfeeding is safe for the infant and represents the most effective means of resolving engorgement and inflammation. Should symptoms persist or worsen after 24 hours of the above non-pharmacological measures, antibiotic treatment is indicated.
The updated ABM protocol reflects a shift away from reflexive antibiotic prescribing for all cases of mastitis. One of the biggest threats to humans is drug resistant infections. Inappropriate prescribing of antibiotics has been the major cause of antimicrobial resistance. The HSE has set a target of reducing the community consumption of antibiotics by eight percent by 2025. However, antibiotics are indicated where there is evidence of bacterial infection, systemic illness, or failure to improve within 24 hours of supportive management. The HSE guidance recommends Flucloxacillin 500mg-1g QDS for five to 10 days depending on symptoms as the first-choice option. Clindamycin 300mg-450mg is the second-choice option or for cases of penicillin allergy. Pharmacists should counsel patients on completing the full antibiotic course and reassure them that the recommended antibiotics are compatible with breastfeeding.
Beyond the dispensing of prescribed medications, pharmacists can provide invaluable support to mothers experiencing mastitis by reinforcing evidence-based advice, addressing concerns about medication safety during breastfeeding and directing patients towards specialist lactation support. Public Health Nurses and Infant Feeding Lactation Specialists represents a vital resource for ongoing breastfeeding support.
Early, informed intervention at the pharmacy counter can prevent escalation of engorgement, ductal narrowing and mastitis to abscess and reduce unnecessary discontinuation of breastfeeding — outcomes that are beneficial for both mother and infant.
References available on request.