

- About Us
- News & Publications
- Conference
- IPU Jobs
- Practice & Support
-
- Safe Pharmacy
-
-
-
Safe Pharmacy | Get Help
Safe Place | Safe phone

-
-
- Professional Academy
- Membership

At a March meeting of the Oireachtas Health Committee, the IPU’s President Dermot Twomey told the assembled TDs and Senators, “As a country, we need to take a more proactive approach to the management of medicine shortages and indeed to pharmaceutical care in general.” Mr Twomey said, “an agreed national strategy for pharmaceutical care” would be a “fundamental and seismic change . . . This would help to deliver better health outcomes for patients. This should be owned by the Minister for Health and driven by the appointment of a Chief Pharmaceutical Officer within the Department.”
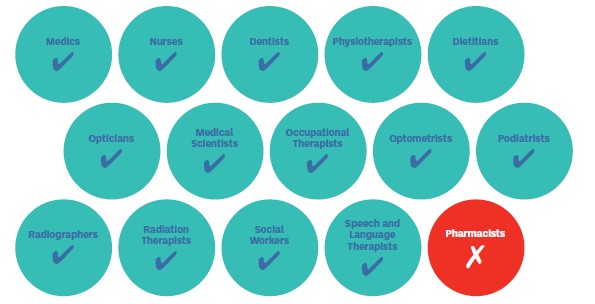
The IPU has long been advocating for the appointment of a Chief Pharmaceutical Officer (CPO), saying it would be a vital step in ensuring a more joined-up strategy for pharmaceutical care, especially given how much the scope of practice for community pharmacists has been expanded in recent years, with even further expansion expected. At present, there is a Chief Medical Officer, a Chief Nursing Officer and a Chief Dental Officer within the Department of Health (see Table 1). A CPO is in place across our neighbouring jurisdictions in Northern Ireland, Scotland, England and Wales, with accompanying strategies driving policy and associated actions.
Table 1: Healthcare professional knowledge at a Chief Officer level in the Department of Health
While there is no such role in Ireland at present, a similar role was in place as recently as 2013.
A Chief Pharmacist was in place in the Department of Health until 2013. Following the appointment of then Chief Pharmacist Marita Kinsella to the role of PSI Registrar in 2013, the Chief Pharmacist role was advertised, but the Department said no suitable candidates were identified at that time, and in 2014 the Department said it remained unable to fill the post.
The Chief Pharmacist was responsible for policy and legislation relating to the regulation of medicines, medical devices, cosmetics, narcotics and psychotropic substances, as well as policy and legislation regulating pharmacists and pharmacies. She also chaired the EU Council working party on pharmaceuticals and medical devices during the Irish presidency of the EU.
In 2014, two pharmacists at Assistant Principal level were recruited by the Department of Health to undertake the duties of the Chief Pharmacist until a suitable candidate was identified. However, the position was never advertised further, and both the IPU and the Hospital Pharmacy Association of Ireland wrote to the Department expressing serious concern at the role not being filled, saying there were many key developments happening at that time that should include the involvement of a Chief Pharmacist.
In response to questions from the Irish Times in August 2014, the Department of Health insisted that it still hoped to appoint a Chief Pharmacist, on the same salary scale as the former post holder. However, the role was never revived.
The IPU strongly advocated for the Chief Pharmacist role to be filled back in 2013, and has continued to assert in the intervening ten years that appointing a CPO will ultimately benefit patient care. But how has this worked in other jurisdictions? The IPU Review spoke with colleagues in Scotland and Northern Ireland to examine what their experience has been.
The CPO role has been in place in Scotland for over 25 years. The role is designated as the professional lead for NHS pharmaceutical care and medicines policy in Scotland, providing advice to the First Minister, the Health Secretary and the wider Ministerial team, and strategic leadership to the pharmacy profession in Scotland.
Community Pharmacy Scotland’s (CPS) Head of Policy and Development Amanda Rae explained that the CPO, “works within the Pharmacy and Medicines Division of the Chief Medical Officer Directorate, which supports close working links and ensures that pharmacy is represented in Scottish Government policy development and delivery. The CPO has a specific pharmacy policy team who work closely with the Community Pharmacy Scotland Board Negotiating Committee on all matters relating to negotiating finance and policy.”
Alison Strath, the current CPS identified her priorities as, “pharmacy’s contribution to the Government’s plans for the Recovery of the NHS in Scotland, the development of the four new Care Programmes and the establishment of the National Care Service. This will mean continuing to develop our community pharmacy services, enabling the transformation of hospital pharmacy and enhancing the role of pharmacy teams in GP practices.” Ms Rae said, “The CPO is visible to the community pharmacy network, in direct communication, in various pharmacy media and in her regular communications with the Scottish Government and CPS negotiating meeting.”
There have been multiple strategy documents from the Office of the CPO, which Ms Rae said, “give a clear direction for all areas of pharmacy, upon which policy and development can be built. From a CPS perspective, this supports our work to continually develop and secure a contractual framework for the provision of pharmaceutical services and care, supported by a sustainable funding model which encourages investment in the network.”
Gerard Greene, Chief Executive of Community Pharmacy NI, explained that the role of CPO has been a long-standing position within the Department of Health in Northern Ireland. Mr Greene said, “having the input of a Chief Pharmaceutical Officer at a strategic level has been very important”; “It is important for the pharmacy profession in any country to have a Chief Pharmaceutical Officer within the Department of Health. In her position as CPO, Prof. Cathy Harrison has the ability to shape policy, develop strategies, as well as guide and advise other senior DoH officials and the Health Minister on pharmacy matters. There is huge potential in having someone with a unique pharmacy perspective in this position as it means that the ability to influence, at the highest level within the Department of Health, is there.”
Mr Greene went on to explain the practical difference this makes to community pharmacists in Northern Ireland: “Undoubtedly having a Chief Pharmaceutical Officer in post has made a difference to pharmacists on the ground, whether they are within the community, hospital, or General Practice settings in Northern Ireland. It means that when issues arise within the pharmacy profession, be that related to policy or strategy, they can be conveyed directly to the Chief Pharmaceutical Officer for consideration and action. The Chief Pharmaceutical Officer currently chairs and/or leads on a number of important policy and development matters, for example, pharmacy workforce, medicines supply and EU exit matters, initial education and training reforms and overall strategy development.”
Mr Greene said that the CPO in Northern Ireland was a strong advocate during the pandemic for the pharmacy profession: “Close collaboration with Cathy and other senior health service officials enabled community pharmacy services to be developed at pace, resulting in the prompt implementation of new services including, the Emergency Supply Service, and the COVID-19/influenza vaccination programme. Furthermore, services which have been introduced during the pandemic have been introduced as routine services in this post-pandemic period.”
While the CPO in Northern Ireland does not publish strategic documents from their office, the Department of Health has produced a number of strategies for the community pharmacy sector, including the 2014 document Making it better through pharmacy in the community, which provided an overarching strategy. Mr Greene says; “In recent years, the emphasis has switched to the development of commissioning plans, and these provided the blueprint for the development of services introduced in response to COVID-19. In a post-pandemic era, I have no doubt that the previous documents will undergo a refresh and moving forward, with a combination of new strategies and commissioning plans, a roadmap for the evolution of community pharmacy and the wider profession will be delivered.”
The IPU’s submission also highlights legislation and policy proposals that will be coming before the Department of Health shortly, which require pharmacist expertise and oversight, see Table 2.
Table 2: Upcoming legislation and policy decisions that require pharmacist expertise and oversight
| Timeline | Event |
| 2023 | Revision of the EU general pharmaceuticals legislation |
| 2023 | FMD legislation Ireland |
| 2023 | HPRA Medicines shortages framework |
| 2023 | Expert guidance on Windsor framework and supply of medicines |
| 2023 | Digital Healthcare Framework |
| 2023 | Health Information Bill |
| 2023 | ePrescribing and National Medicinal Products Catalogue development and shared care records |
| 2023 | Expert Taskforce to Support Expansion of Pharmacists Roles |
| 2024 | EU general pharmaceuticals legislation |
| 2025 | Implementation of Windsor framework and supply of medicines |
| 2025 | EU general pharmaceuticals legislation |
| 2026 | EU presidency Q3 & 4 |
Referencing the experience of our near neighbours, Ms Fitzell says the absence of an Irish CPO makes us an outlier in modern healthcare systems, and that absence has been notably felt in many health policy issues, including during the pandemic: “There was an inexplicable delay enlisting community pharmacy as part of the COVID-19 national vaccination campaign. This delay was then repeated when it came to the booster campaign, when pharmacists were initially not included for no logical reason, and despite the clear demand within our local communities. It is logical to suggest that the delayed pharmacy involvement in the COVID-19 vaccination programme rollout would not have happened had a CPO been in place.”
Proposals from the IPU on potential key responsibilities for a CPO are included in a sidebar in this article.
We asked the Department of Health if there are active proposals to reinstate the role of CPO, and we received the following: “Currently there are no active proposals to develop a Chief Pharmaceutical Officer role in the Department of Health. A number of units within the Department have responsibility for advancing policy in key areas of our health system. They are cognisant of potential deliverables that can be realised by and through pharmacists and pharmacy services, to deliver patient centred care in line with the vision of Sláintecare.”
Read the full reply from the Department of Health, and statements from political parties regarding their support for the appointment of a CPO, over the following pages.
The IPU continues to strongly advocate that a Chief Pharmaceutical Officer be appointed as a matter of urgency.
The role of Chief Pharmaceutical Officer at Assistant Secretary level would have a full policy brief and cover the following roles and responsibilities:

The IPU is calling for the immediate appointment of a Chief Pharmaceutical Officer to deliver pharmaceutical care for our population and ensure:
“ The complexity and bureaucracy of our system is one of the main reasons Ireland often lags behind other countries in the introduction of new medications to treat patients. When there is no single individual with oversight of the entire sector, it is easy to see how it fails to evolve.”





