Key facts:
Bowl cancer, or Colo-Rectal Cancer (CRC) is the fourth most common invasive cancer in Ireland, with approximately 2,600 new cases diagnosed annually in this country. However, it is the second most common cause of cancer death, after lung cancer, with just over 1,000 deaths every year.
Men are more likely than women to develop CRC in Ireland; the cumulative lifetime risk of being diagnosed with CRC for a male in Ireland is 1 in 14, and for a female is 1 in 19.
Survival from CRC is markedly higher in people who are diagnosed when the disease is at an early stage; stage I disease has a five-year survival rate of over 98 per cent, while survival at stage IV disease falls to just 14.6 per cent.
Figure 1: Colo-rectal cancer five-year survival in Ireland by stage at diagnosis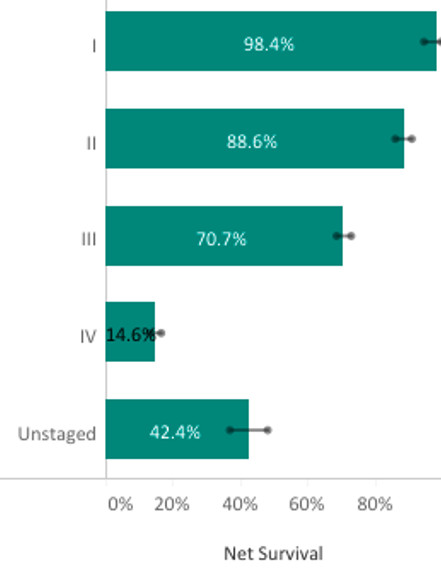
Unfortunately, a minority of cases of CRC in Ireland are diagnosed at an early stage — approximately 40 per cent of cases are diagnosed at stage I & II, with the remainder being diagnosed at late-stage, more advanced disease.
Although there appears to be no relationship between deprivation and CRC incidence in Ireland, deprivation is linked with poorer survival from this disease; patients from the most deprived group show significantly poorer survival relative to the least deprived group. In addition, urban patients from the most deprived group were significantly more likely (+20 per cent in relative terms) to be diagnosed at a late stage (stage IV) compared with the least deprived group.
Approximately 75 per cent of cases of CRC are sporadic. The remaining 25-30 per cent of cases are thought to be linked to non-modifiable risk factors such as a personal history of polyps or adenoma, a family history of colorectal cancer, or hereditary risk (for example, Lynch syndrome or familial adenomatous polyposis).
According to the World Health Organisation, 30-50 per cent of cancers overall are preventable. There are steps people can take to reduce their risk of developing CRC.
Obesity is associated with an increased risk of developing CRC compared with normal-weight individuals. Lack of dietary fibre, and consuming a diet high in processed and red meat also increases risk. Physical activity, however, reduces the risk of developing the disease and also reduces the risk of recurrence after treatment. Patients should be encouraged to maintain a healthy weight, engage in physical activity, avoid alcohol, red and processed meat, and consume a diet high in wholegrain, wholemeal, fruit, and vegetables.
Human Papilloma Virus (HPV) has a causal role in the development of anal cancer. The HPV vaccine is available free of charge to all first-year secondary school students. However, national uptake of the HPV vaccine is around just 75 per cent, well below the target of 90 per cent. HPV should be recommended to all first-year second-level students.
Increasing age is a major risk factor for CRC, with 90 per cent of cases in Ireland occurring in people aged over 50 years. Males are slightly more likely to develop the disease than females.
For those with a first degree relative with CRC (i.e. parent, sibling, or child) the relative risk of developing the disease is 2.24, increasing to 3.97 if two first degree relatives are affected. Certain inherited conditions such as Lynch Syndrome, Familial Adenomatous Polyposis, and hamartomatous polyposis syndromes also increase risk.
Inflammatory bowel disease (IBD), which includes Crohn’s Disease and Ulcerative Colitis, is a chronic, progressive disease of the gastrointestinal tract. People with IBD are not only more likely to develop CRC, but also more likely to develop it at a younger age.
It is important to note that no screening test is 100 per cent accurate. ‘False negative’ results may occur, where the screening test is negative but the person does, in fact, have cancer. Thus, negative screening test should not preclude appropriate investigation in a patient with symptoms suspicious for cancer.
Rectal bleeding is a common presenting symptom of CRC. While most people with rectal bleeding will turn out not to have CRC, about 40 per cent of people with CRC will have rectal bleeding. Increased frequency of bowel motions, with looser stool can occur, particularly in left-sided CRC. Constipation, on the other hand, has a low predictive value for CRC. Loss of weight, malaise, fatigue (due to iron-deficiency anaemia) and abdominal pain and/or swelling can also occur. Patients who develop any of these symptoms should be encouraged to seek medical advice as soon as possible given the substantial survival benefit associated with early diagnosis of CRC.
While absolute numbers remain low, incidence rates of CRC are rising in younger people, aged less than 50 years, in the developed world. This appears to be largely driven by increasing incidence in the US, Australia and Canada. The reasons for the increase in young-onset CRC are not fully understood — it is important to note that the majority of cases (up to 75 per cent) occur in people with no family history of the disease. Contributing factors to the increasing incidence of young-onset CRC may include the Westernised sedentary lifestyle and diet, increased antibiotic use, and obesity. In Ireland, about 10 per cent of cases of CRC occur in people under the age of 50 years. Although this represents a small minority of the overall number of cases, it is important to remember that people are never ‘too young’ to develop cancer, to be vigilant for symptoms of CRC in young people, and to promote a healthy lifestyle in all age groups.
Iron-deficiency anaemia, where anaemia occurs in the presence of low serum Ferritin, may occur in CRC, and should prompt further investigation. Other blood-based markers, such as carcino-embryonic antigen (CEA) and cancer antigen CA19.9 may be used in the surveillance of disease post-treatment but are not sufficiently reliable to aid diagnosis.
Colonoscopy is the primary investigation, and allows a tissue diagnosis. CT colonography is the radiological investigation of choice when colonoscopy is contraindicated.
Patients with suspected CRC may be referred by their GP for direct-access colonoscopy (where available) or to a colorectal or gastroenterology outpatient department for urgent review.
For localised CRC, surgery to remove the tumour, is the mainstay of curative treatment. Pre-operative neo-adjuvant and post-operative chemotherapy and/or radiotherapy may also be required. The chemotherapy treatment regimen to be used should take into account factors such as histology, molecular pathology, age, patient’s performance status, comorbidities and the patient’s preference. Details on the preferred chemotherapy treatment regimens in Ireland can be found on the NCCP website at hse.ie/cancer.
Patients who have had potentially curative surgical treatment for non-metastatic colorectal cancer are typically offered follow-up for detection of local recurrence and distant metastases for the first three years. Follow-up may include serum carcinoembryonic antigen (CEA) and CT scan of the chest, abdomen and pelvis. Patients with more advanced disease may require more frequent surveillance.
At all stages on their cancer journey, patients should be encouraged to engage in physical activity which has been shown to reduce risk of developing CRC, and reduce risk of recurrence of disease. Patients who smoke tobacco products can be encouraged to quit, as quitting, even during and after treatment is beneficial. Free support to help people quit smoking is available at quit.ie.
Colorectal cancer is one of Ireland’s most common cancers. It is crucial that people take steps to reduce their risk of this disease, including participating in Bowelscreen and adopting a healthy lifestyle. If symptoms do occur, it is vital to seek medical advice as soon as possible; CRC is highly treatable if it diagnosed at an early stage.
“Bowel screening can both prevent CRC by detecting pre-cancerous growths which can be removed before they develop into cancer, and can also detect CRC at an early stage in people who are asymptomatic, when cure rates are significantly higher.”
References available on request.
The NCCP has developed a suite of resources for the public and healthcare professionals to help increase awareness of cancer. These include an ‘Early Diagnosis of Cancer’ e-learning module and ‘Reduce your risk of Cancer’ e-learning module on HSELand (hseland.ie). These are available free of charge and can be accessed by clicking on the ‘Cancer’ tab on the HSELand website.
The Irish Institute of Pharmacy (IIOP) have created a Cancer Care Hub, created for pharmacists in collaboration with the National Cancer Control Programme (NCCP). This resource signposts pharmacists to information to support patients in the prevention, early detection, treatment and navigation of life after cancer.
Cancer-related posters, leaflets, and information booklets are available on healthpromotion.ie. These can be downloaded and printed, or alternatively, hard copies can be ordered and delivered free of charge.
The Community Pharmacy Agreement 2025 is designed to support the delivery of safe, equitable, and efficient healthcare, and to ensure that community pharmacists are better equipped to contribute to national health priorities such as Bowelscreen.
Community pharmacists and their teams, as trusted healthcare professionals, can play an important role in supporting increased uptake of the Bowelscreen Programme through promoting the programme at population level as well as enhancing access by supporting individuals to participate in the programme.
Under CPA25, expanded participation in national programmes such as BowelScreen will be rolled out in 2026.