



Learning outcomes:
By the end of this article, you should be able to:
Chronic insomnia is defined as a subjective, long-term difficulty falling asleep, staying asleep, or having poor sleep quality (early morning awakening) that persists for at least 3 months, occurs 3 or more times per week, and is accompanied by significant daytime impairment or distress, despite having adequate opportunity for sleep.
The Core Symptoms are difficulty initiating sleep, maintaining sleep, or early morning awakening followed by daytime consequences of fatigue, irritability, mood alteration, cognitive impairment (concentration/memory issues), or reduced performance. The duration threshold is at least 3 times per week for at least 3 months.
Globally, among adults, approximately 10–30 per cent report insomnia symptoms (trouble falling asleep, staying asleep, or poor sleep quality), and 6–10 per cent meet criteria for chronic insomnia disorder (symptoms ≥3 nights/week for ≥3 months, with daytime impairment). Acute insomnia affects 30–50 per cent of adults at some point, often during stress, illness, or major life changes. Insomnia is more common in women than in men, and prevalence increases with age. Unfortunately, the prevalence is higher in people with depression, anxiety, chronic pain, sufferers of cardiovascular disease, and among shift workers.
Chronic insomnia has been linked firmly with significant medical morbidity, such as cardiovascular disease. Several epidemiological surveys have demonstrated a significant association between difficulty initiating sleep or poor sleep quality and adverse cardiometabolic outcomes, including hypertension and diabetes.
Individuals with insomnia exhibit small-to-moderate impairments in cognitive performance, particularly in working memory, episodic memory, and selected aspects of executive functioning.
It has been established that insomnia is highly comorbid with psychiatric disorders and is a risk factor for the development of depression, anxiety, and suicide.
Insomnia imposes substantial economic costs, including direct healthcare expenditures across multiple sectors, indirect costs related to accidents, absenteeism, and reduced work productivity, as well as additional related costs that do not fall strictly into direct or indirect categories. Collectively, these direct, indirect, and related costs were conservatively estimated at US $30–35 billion annually in the United States. Evidence suggests that significant economic gains may be achieved through the outpatient management of insomnia in specialised sleep centres.
Insomnia can be classified in several complementary ways: by duration, cause, pattern of sleep disturbance, and specific clinical subtypes.
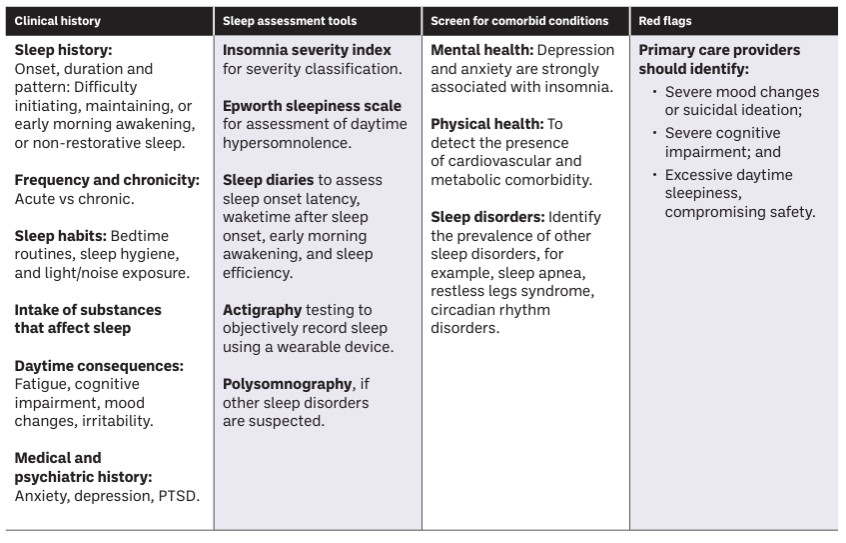
Insomnia is a common and often under-recognised condition in primary care. A structured assessment is essential to determine severity, identify underlying causes, evaluate daytime impact, and guide targeted management, including behavioural strategies, lifestyle modifications, and pharmacological interventions when appropriate.

Pharmacists, in collaboration with physicians and other healthcare professionals, occupy a unique role in supporting patients with sleep disturbances. As accessible healthcare providers, pharmacists help bridge the gap between self-management and medical care, ensuring that patients receive timely interventions and appropriate referrals when necessary.
Pharmacists are best placed to screen patients for insomnia when they present to pharmacies with sleep difficulties. Screening and categorising insomnia into acute/situational or chronic insomnia is often helpful to identify the pathway to proceed with. This can be education and counselling on sleep hygiene, use of over-the-counter medications which can help to reestablish normal sleep patterns (based on the currently available recommended guidelines), or advising on referral pathway and collaborating with other healthcare professionals. The pharmacists also play a role in the monitoring of patients who are on pharmacological treatment of chronic insomnia.
The pharmacies can also play a vital role in sleep education and enforcing the importance of obtaining a good night’s sleep. Once the pharmacist identifies that the patient’s symptoms are consistent with insomnia, the patient can be encouraged to adopt optimal sleep-related behaviours and be educated about the homeostatic sleep drive. The pharmacist can also consider including this content in an in-service programme for the wider pharmacy team.
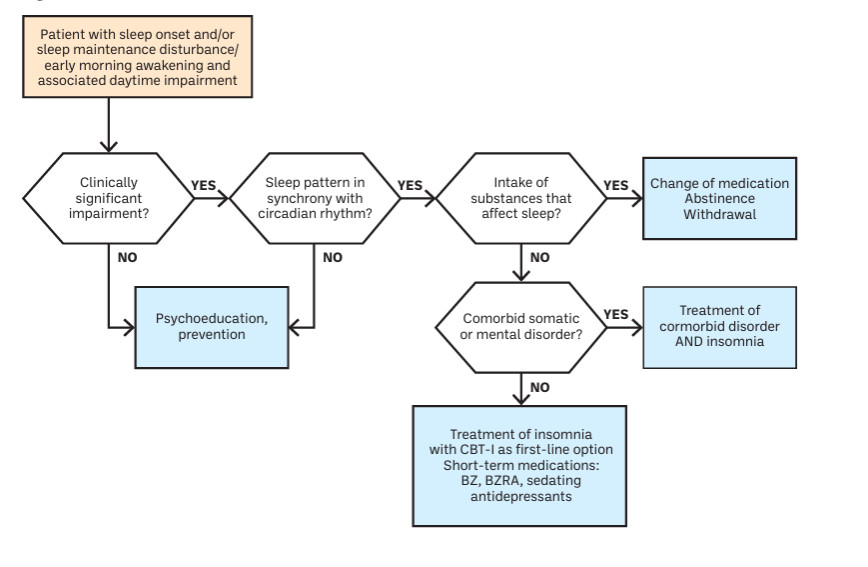
Cognitive-behavioural therapy for insomnia (CBT-I) is the most effective nonpharmacological treatment for chronic insomnia. Its outcomes are comparable to those of sleep medications, but without any associated side effects. CBT-I is also linked to lower relapse rates, and improvements in sleep often persist and continue to increase well after treatment has ended.
CBT-I is the recommended first line treatment for insomnia and pharmacological treatment for insomnia is only to be considered when CBT-I is not easily available or when it is not successful.
Cognitive behavioural therapy for insomnia typically includes components such as psychoeducation and sleep hygiene, relaxation techniques, stimulus control therapy, sleep restriction therapy, and cognitive therapy. Usually, CBT-I is applied face to face (either on an individual basis or in a group format) by a trained clinician in four-eight sessions.
Psychoeducation/sleep hygiene: Psychoeducation focuses on education regarding sleep hygiene practices, including health-related behaviours (for example, clock-watching, exercise, substance use) and environmental factors (for example, light, noise, temperature) that may facilitate or impair sleep. It also includes information about normal sleep physiology and age-related changes in sleep.
Relaxation therapy: Relaxation interventions target the reduction of physiological and cognitive arousal at bedtime and include techniques such as progressive muscle relaxation, autogenic training, imagery, and meditation.
Behavioural strategies (sleep restriction and stimulus control): Sleep restriction therapy aims to consolidate sleep by limiting time in bed to the individual’s actual sleep duration. Stimulus control therapy employs behavioural instructions to re-associate the bed and bedroom with sleep and to establish a consistent sleep–wake schedule.
Cognitive therapy: Cognitive therapy involves identifying and modifying dysfunctional beliefs, misconceptions, and maladaptive cognitions related to sleep, insomnia, and its perceived daytime consequences.
Cognitive behavioural therapy for insomnia, though being the first-line treatment for insomnia, is not easily available despite its effectiveness and clinical validity. Thus, the widespread implementation of CBT-I will be a major challenge for the future.
“Cognitive-behavioural therapy for insomnia (CBT-I) is the most effective nonpharmacological treatment for chronic insomnia.”




