Emergency contraception is indicated to reduce the risk of a pregnancy occurring following unprotected sexual intercourse (UPSI) or failure of contraception. There are three types of emergency contraception:
- copper intrauterine device (copper-IUD);
- ulipristal acetate 30mg tablet; and
- levonorgestrel 1.5mg tablet.
The two oral emergency contraceptives, ulipristal acetate and levonorgestrel, can be accessed in most community pharmacy settings, following a consultation with the pharmacist. As clinical guidelines are regularly updated, this article summarises the considerations a pharmacist can have when choosing the most appropriate action for a woman seeking emergency contraception.
Emergency contraception is indicated after unprotected sexual intercourse (UPSI). There is a possibility of pregnancy following UPSI anytime from day 21 after childbirth (unless the woman is fully breastfeeding and amenorrhoeic, in which case pregnancy is possible for months after childbirth). Pregnancy is also possible from five days after a miscarriage, abortion or ectopic pregnancy. Emergency contraception may also be required if regular contraception has become compromised, but it is important to obtain a full history regarding the contraception use and the reason for the woman presenting for emergency contraception to fully understand if emergency contraception is indicated (more later).
Even though a copper-IUD cannot be placed by a pharmacist, it does still merit a mention here. It is the most effective form of emergency contraception, with a reported effectiveness rate of >99.9%. One of the main points to remember about a copper-IUD is that it is the only form of emergency contraception to be effective after ovulation. Therefore, as a community pharmacist, if there is a possibility that the woman has ovulated prior to presenting to the pharmacy, this must be explained to the woman, and she should be signposted to a provider of the copper-IUD. Guidelines from the Faculty of Sexual and Reproductive Health (FSRH) which are a UK-based, National Institute for Health and Care Excellence (NICE) accredited group, state that all women seeking emergency contraception should be advised that a copper-IUD is the most effective method of emergency contraception. The FSRH guidelines suggest that all providers of emergency contraception, should signpost all women looking to access emergency contraception, to a provider of the copper-IUD. However, the guidelines also advise that even if you refer a woman to have a copper-IUD placed, oral emergency contraception should also be provided at the time of signposting, in case the woman changes her mind. It is also worth remembering that according to the Summary of Product Characteristics for each of the oral emergency contraceptives state that they can be taken ‘at any time during the menstrual cycle’.
The two oral emergency contraceptives work by the same mechanism — delaying ovulation. This means two main things: (i) ovulation is still likely to occur in the cycle after emergency contraception has been taken, just at a later date, and (ii) oral emergency contraception does not work after ovulation has occurred. A pharmacist will need to establish that a woman is likely to be in the part of her cycle before ovulation has occurred, by asking questions such as ‘when was your last period?’, ‘is your cycle regular?’ and ‘if your cycle is regular, how many days apart are your periods approximately?’. Once it has been established that the woman is likely to be in the part of her menstrual cycle prior to ovulation, some other questions can help establish whether levonorgestrel or ulipristal acetate will be more suitable.
It is imperative that pharmacists providing emergency contraception have an understanding of the hormones and key timings of the menstrual cycle (Fig. 1). Luteinising hormone (LH) provides the trigger for ovulation, and both levonorgestrel and ulipristal acetate work by suppressing the luteinising hormone peak, which delays ovulation by approximately five days. In a natural menstrual cycle (no hormonal contraceptives), a pregnancy is most likely to happen if UPSI occurs in the five days before ovulation or on the day of ovulation — this is considered to be the highly fertile time of a woman’s cycle. The reason for this is that sperm are viable in the female genital tract for about five days, whereas the egg is viable for less than one day.
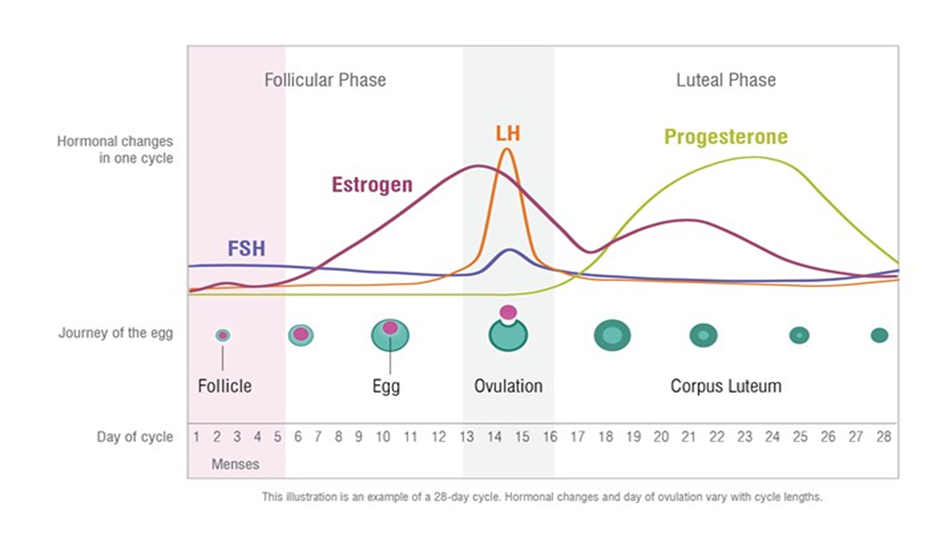
Fig. 1: Natural Menstrual Cycle
Levonorgestrel
Levonorgestrel is a progestogen which acts by suppressing the LH peak. This delays, or in rare instances blocks, ovulation for five days. Levonorgestrel is less effective than ulipristal acetate in the highly fertile period, as levonorgestrel must be taken prior to the start of the LH surge. Levonorgestrel can be used if UPSI occurred within the last 72 hours and is the preferred choice in a few different situations:
- Patients who are already taking a progesterone/progestogen (such as those found in contraceptives and hormone replacement therapy);
- Patients who require a quick initiation of regular hormonal contraception in the days after emergency contraception;
- Patients who are breastfeeding, as available limited evidence suggests no effect on the baby. To minimise levels of drug in breastmilk, patients can be advised to take the tablet directly after breastfeeding and to avoid nursing for eight hours; and
- For patients taking concomitant enzyme-inducing drugs, or who have taken enzyme inducing drugs in the last four weeks, a double-dose (3mg total dose) of levonorgestrel can be provided to patients. This double-dose is in the Summary of Product Characteristics and is also mentioned in the PSI Guidance and the FSRH Guidelines. A double-dose of levonorgestrel is the only option available from pharmacies which is suitable for patients on enzyme inducers. Patients should be informed that the effectiveness of the regimen is unknown and that a copper-IUD is the most effective form of emergency contraception.
Ulipristal Acetate
Ulipristal acetate is a progesterone receptor modulator which acts by suppressing the LH peak. Similar to levonorgestrel, this delays ovulation by at least five days. Ulipristal acetate is approximately 98.5% effective up to 120 hours post UPSI and is considered to be more effective than levonorgestrel. It has one major drawback — it interacts with other progesterone/progestogen containing products. This means that if a woman seeking emergency contraception has taken medicine containing progesterone or progestogen (including contraception, hormone replacement therapy (HRT) and others) in the seven days prior, or will be taking such medicines in the five days after emergency contraception, the effectiveness of ulipristal acetate can be compromised. This means that for any patient who requires emergency contraception and who is on hormonal contraception will need to delay restarting their hormonal contraception/HRT for five days after taking ulipristal acetate. Additional precautions, such as the use of a condom, will be required by all patients after taking oral emergency contraception. The time to contraceptive cover being re-established from hormonal contraception is as per the Summary of Product Characteristics for each individual hormonal contraceptive (generally two days for progestogen-only pill, seven days for combined hormonal contraception, and nine days for Qlaira).
Due to its superior effectiveness, ulipristal acetate is the preferred choice of oral emergency contraception in the following circumstances:
- Patient is very close to time of ovulation (during the highly fertile time);
- *Patients who weigh >70kg or have a body mass index (BMI) of >26kg/m2; and
- *There is conflicting advice regarding the effectiveness of oral emergency contraception in those who are over 70kg or those who have a BMI of >26kg/m2. The European Medicines Agency (EMA) and subsequently the PSI have both stated that the evidence about reduced effectiveness of oral emergency contraception in individuals who weigh >70kg or have a body mass index (BMI) of >26kg/m2 is not conclusive. The PSI emphasise the importance of providing emergency contraception as soon as possible after UPSI. The FSRH suggest using ulipristal first line and a double-dose of levonorgestrel second line. However, a recent study investigating if there was any difference in effect of levonorgestrel 1.5mg or levonorgestrel 3mg on follicle rupture concluded that there was no significant difference. Thus, on balance, in Ireland, the guidance is to provide emergency contraception as soon as possible. Patients who are overweight should first be signposted for a copper-IUD placement, as weight has no effect on the efficacy of a copper-IUD. The preferred oral emergency contraceptive, if suitable, is ulipristal acetate. If ulipristal acetate is not suitable, levonorgestrel 1.5mg could be offered.
With either form of oral emergency contraception, serious side-effects are rare. The side-effects commonly experienced include headache, nausea and dysmenorrhoea. If a patient is so nauseous that they vomit within three hours of taking oral emergency contraception, a further dose of the same oral emergency contraceptive as was given originally, should be dispensed. As both oral emergency contraceptives work by delaying ovulation, both have the side-effect of delaying menstruation. Every patient should be advised to take a pregnancy test if their period is delayed by more than seven days. However, it is useful to know that 20% of patients who took ulipristal acetate have a delay of more than seven days to their period, as do 10% of patients who took levonorgestrel. There are two specific circumstances in which ulipristal acetate is unsuitable due to drug-drug interactions:
- Patients who take drugs which increase gastric pH: effect on ulipristal acetate efficacy is unknown. A copper-IUD or levonorgestrel should be offered instead; and
- Patients who have severe asthma requiring oral glucocorticoids: ulipristal acetate has an antiglucocorticoid effect. A copper-IUD or levonorgestrel should be offered instead.
Conclusion
Finally, as oral emergency contraceptives delay ovulation, there is the possibility that women may require emergency contraception twice in one cycle. The general recommendation is that if levonorgestrel is provided the first time it is required in a cycle, levonorgestrel should be provided again after the second instance of UPSI and similarly for ulipristal acetate. It is also important to remember that oral emergency contraceptives are not harmful to a very early pregnancy.
Pharmacists will need to structure any consultation with a woman requesting oral emergency contraception to ensure that they gather all the relevant information to consider all of the factors mentioned above: time since UPSI, use of other hormone-containing medicines, possible drug-drug interactions, other factors affecting choice of emergency contraception (breastfeeding for example).








